
What is nearsightedness?
Updated JUN 5, 2023 • 7 min read


Summary in 30 seconds:
What is nearsightedness? In this article, we’re going into detail about this common vision condition, its causes, and the recommended eyewear solutions used to correct it.
How does nearsightedness “work”?
Nearsightedness, also known as myopia, is a common condition that affects approximately 40% of Americans [1].
In this article:
- How does nearsightedness “work”?
- Diagnosing nearsightedness/myopia.
- What causes nearsightedness?
- What type of lens is used to correct nearsightedness?
- What about refractive surgery?
How does nearsightedness “work”?
Looking at a clock across the room or at a sign on the freeway requires clear distance vision. The nearsighted person has difficulty with distant vision. Seeing distant objects may be even more difficult when there is dim lighting. However, a nearsighted person may find reading a book or working on the computer to be perfectly clear.
Nearsightedness & the eye’s structure.
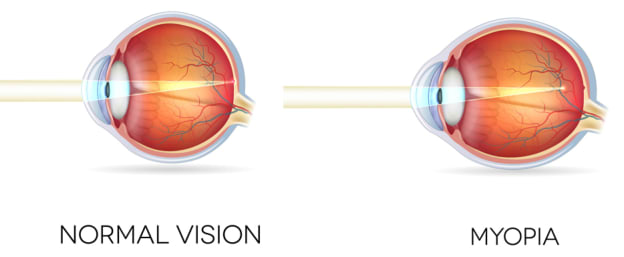
The eye is designed to collect and focus light information that is then sent to the brain for interpretation. Light is mainly focused by the cornea and the lens inside the eyeball. The focal point of this light should land on the retina. The retina is the light sensitive tissue that lines the inside of the eyeball.
A nearsighted eye has a focus point in front of the retina. Nearsightedness occurs when there is a mismatch in the focusing power of the lens and cornea with the length of the eyeball that leads to a focal point in front of the retina. Frequently, a nearsighted eye will have a cornea that is too steep in curvature or too long in length.
Myopia is normally considered a focusing condition and not a disease. A mild amount of myopia is known as common or low myopia. A larger amount of myopia is known as high myopia.
Highly myopic eyes are frequently longer and/or larger. There is a rare form of myopia that is inherited and progressive. Progressive myopia is associated with retinal detachments, cataracts and glaucoma.
Diagnosing nearsightedness/myopia.
Myopia is diagnosed with a comprehensive eye examination by an eye doctor either an optometrist or ophthalmologist. A standardized eye chart is used to measure acuity (the ability to see at a specific distance). Both distance and near vision are checked.
A special light is shone into the eye; light then reflects off the retina and can determine nearsightedness as well as other vision conditions. This test is known as retinoscopy.
This same concept is utilized by an instrument known as an autorefractor which gives a quick assessment of the eye’s focal point. A phoropter is then used to quantify the amount of prescription needed to correct the vision.
Examining more than “just” nearsightedness.
The eyes are also checked to assess if they are working as a team for comfortable binocular vision. This is especially important for children. Children should get a full examination before they start school. Symptoms of squinting, eyestrain, headaches and difficulty seeing objects others can see are all indicators that a child needs their eyes examined.
Besides diagnosing myopia, the doctor will assess the health of the eyes. Are there cataracts? Are the retina and other internal structures healthy? Is the intraocular pressure in a healthy range? Health conditions affecting the body may be evident in the eyes such as diabetes and high blood pressure.
What causes nearsightedness?
The eyes grow rapidly the first couple years of life, slowing down through the school years to reach adult-size in late teens. During this growth period is typically when myopia develops, although adult onset does occur [2]
Genetics certainly plays a role in the development of myopia. The risk for developing myopia increases with a family history of myopia especially with high myopia and progressive myopia.
An increase in nearsighted people.
Prevalence of myopia has increased from 25% of the population in the United States in 1971 to 41.6% in 2017. This increase is occurring worldwide especially in Southeast Asia. The dramatic increase in nearsightedness prevalence likely indicates environmental influences also play a role in the development of myopia.
Since high myopia increases the risk for retinal detachment, cataracts and glaucoma, it begs the question: Is it possible to slow the progression of myopia?
Funded by the National Eye Institute (NEI), the CLEERE study followed 1,200 children ages 6 – 14. It found children who spent more time outdoors had less risk of becoming nearsighted.
Other studies are looking at ways to slow the progression of myopia using specially designed dual-focus daily disposable contact lenses, orthokeratology, bifocal glasses and low dose atropine eye drops [3,4,5].
Nearsighted vision changes.
Vision fluctuations may occur with poor metabolic blood sugar control such as with pre-diabetes and diabetes. Frequently these visual fluctuations are toward nearsightedness. Certain types of cataracts are associated with a myopic shift requiring more frequent prescription changes until cataract surgery is needed. The eyes need to be examined by a doctor if visual fluctuations are occurring.
Nearsightedness may be associated with various genetic syndromes such as autosomal recessive congenital stationary night blindness, retinitis pigmentosa, cone-rod dystrophy and Marfan’s syndrome.
What type of lens is used to correct nearsightedness?
Lens power is measured in diopters (D). The higher the number the more powerful the lens is.
Lenses that correct for nearsighted eyes have a minus sign before the number of diopters, for example -1.00D. A -6.00D lens is stronger than a -1.00D lens. The more powerful the lens that is needed to correct vision, the thicker the lens will be. Low or simple myopia is less than -6.00D. High myopia is greater than -6.00D.
There are lens options available to make vision clear, comfortable and appropriate for age and activities. When selecting the most appropriate correction for nearsightedness, it is important to keep a variety of factors in mind.
Has the correction been prescribed for full time or part time wear?
When a full time prescription is needed, it may be most convenient to consider photochromic lenses. These lenses darken in sunlight and most brands block UV light but vary with the manufacturer.
A multifocal lens may be a good option for full time wear. Multifocal lenses are designed for clear vision at multiple distances. Part time wear tends to be use-specific such as computer/office glasses, driving at night, safety glasses and sporting glasses.
 Square
Square
 Cat eye
Cat eye
 Oversized
Oversized
 Rectangle
Rectangle
 Aviator
Aviator
 Round
Round
How strong is the prescription?
With a more powerful prescription, the lenses are thicker and heavier. One option to help with this is a high-index lens which allows for thinner lenses. Choosing glasses frames that are smaller for higher prescriptions will also help to keep the glasses more comfortable.
Is the correction a multifocal prescription?
A multifocal lens is most commonly prescribed for patients over 40. Sometimes youngsters are prescribed bifocals in hopes of slowing down myopia progression. For safety reasons, children are commonly given polycarbonate plastic lenses. Polycarbonate lenses are very impact resistant.
Is the correction needed for a particular purpose?
The conditions under which people may experience nearsightedness (or at differing levels) may require different solutions.
- Some people experience more nearsightedness at dusk and/or at night. Night driving glasses make for a safer commute.
- Polarized lenses for daylight driving cut the glare.
- Computer glasses are designed for seeing clearly at approximately arms length.
- Glasses for a particular sport are often needed. Besides clear vision, skiing requires sunglasses and/or ski goggles to protect the eyes from high intensity light damage. For sports like tennis and baseball, a wrap-around lens design helps to cut down glare.
- Welding requires special filtering lenses with a face shield. Prescription safety glasses and goggles are available and should be worn for protection.
What type of lens coating should be considered?
An anti-scratch coating is recommended for plastic lenses. A UV-coating is clear yet filters out UV rays. For computer use, consider using a blue light filtering coating. An anti-reflective coating reduces glare during the day and halo-like effect around lights at night.
Are contact lenses an option?
Contact lenses are designed and used for many reasons including:
- For daily wear as an alternative to glasses
- Bandage lenses post-surgery and post-injury
- For sports when glasses fog up or when peripheral vision is extra important
- Specialty scleral lenses for corneal irregularities, keratoconus and severe dry eye.
Contact lenses may be prescribed in an effort to slow the progression of myopia with gas permeable semi-rigid lenses, dual-focus daily disposable contact lenses or orthokeratology.

What about refractive surgery?
The amount of myopia correction and the thickness of the cornea will influence the type of surgical options for an individual. Other considerations influencing surgical options include irregular corneal shape, severe dry eye, early cataracts and age. Discuss with an eye doctor if refractive surgery could be considered.
LASIK (laser-assisted in situ keratomileusis) surgery to correct myopia is a popular option. The surgeon creates a flap in the cornea then using a laser reshapes inner corneal tissue then replaces the flap.
PRK (photorefractive keratectomy) laser surgery reshapes corneal tissue from the surface of the cornea. A flap is not created.
ICL (Implantable Collamer lens) When the cornea is too thin for the amount of nearsightedness correction needed, a surgeon may be able to implant a corrective lens in front of the natural lens.
In summary – get your eyes checked, frequently.
Regular eye examinations are important for maintaining the health of your eyes and the quality of your vision [6]. As a guideline, the eyes should be checked at six months of age, 3 years old, before starting school, and then every 2 years until 60 years old.

After 60, the eyes should be examined annually. If there are general or eye health conditions like glaucoma, diabetes, hypertension, certain long term medications, the frequency of eye examinations may need to be increased.
Published March 1, 2023|Updated June 5, 2023
SOURCES

